
Roux-en-Y Gastric Bypass
Rou-En-Y Gastric Bypass is a bariatric surgical procedure. The bariatric surgeons highly recommend this method in light of its positive effects. The excessive weight loss after this surgery is higher in a compliant person than with restrictive procedures. Dr. Deepak, the best bariatric surgeon in Chennai extends his services to imbibe a transformation in the lives of his patients. Through his expertise, we are competent to provide quality bariatric surgery in Chennai exclusively at our clinic.
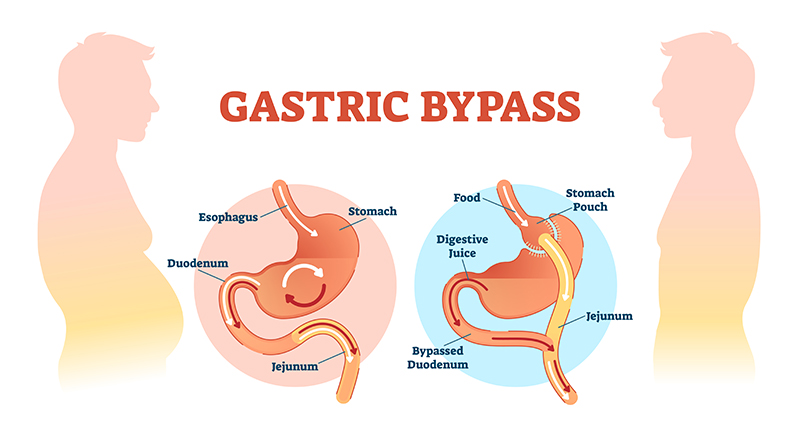
The Roux-en-Y gastric bypass is considered as the gold standard of all bariatric surgeries. This is due to the dual benefits of restriction and malabsorptive components of the procedure. Dietary restrictions are significant because the procedure leaves only about 20 mL of gastric pouch in volume. The outlet is so small that a sensation of satiety is created upon distention of food. Intentional malabsorption is created due the separation of food. This food passes from the biliopancreatic secretions and through the alimentary limb of Y.
Technique
- Small incisions in the abdominal wall facilitate the insertion of trocars through which surgical instruments are passed for optimal access to the abdominal cavity.
- After insufflating the abdomen with CO2 gas, the abdominal structures are viewed through the laparoscope.
- The omentum and transverse colon are mobilized.
- The ligament of Trietz, which is a connection between the duodenum and the diaphragm, is identified.
- The transverse mesocolon is lifted to create a window.
- Upon visualizing the undersurface of the stomach, the jejunum is divided into the biliopancreatic limb and the Roux-limb.
- The Roux-limb forms the alimentary limb because of its connectivity to the pouch of the stomach.
- The shorter part is the biliopancreatic limb also known as the biliary limb.
- Measurement of 100 cm to 150 cm of the jejunum will decide the length of the alimentary limb.
- The longer measured portion is anastomosed by sewing it to the shorter part of the jejunum. This part of the procedure is known as jejunojejunostomy.
- The distal end of the Roux limb and the biliopancreatic limb are connected with suturing and stapling.
- An internal hernia can be avoided by closing the mesenteric defect.
- Right below the area of attachment (about 1 – 2 inches) between the stomach and the oesophagus, the stomach is divided.
- The lesser curvature of the stomach is reached.
- The lesser sac is accessed through the space behind the stomach.
- The upper section of the stomach that is connected to the oesophagus is called the gastric pouch.
- Approximately 1 – 2 ounces of food is held in the gastric pouch.
- The Roux limb is pulled to be attached to the gastric pouch.
- The jejunum and stomach are sewn or stapled together in about 1 to 2 layers.
- Roughly there is 1 cm of an opening between the intestine and the gastric pouch.
- Redundant Roux limb is reduced, and sutures in an interrupted fashion are placed closing the mesocolon and the Petersen’s defect.
We conduct thorough leak tests to examine the security of the connections and only then closes the incisions.Avail the finest obesity treatment in Chennai at our brand-new center.
Ask doctor
Testimonials
 Very practical approach to my dads gallbladder stone problem .. Surgery was explained well by diagrams and he performed the surgery by key holes which made it pain free for my dad . I had consulted many in the last 1 month including
Very practical approach to my dads gallbladder stone problem .. Surgery was explained well by diagrams and he performed the surgery by key holes which made it pain free for my dad . I had consulted many in the last 1 month including 
Subramanian
Read More The doctor was helpful. He worked with me to select the best option for treatment and helped finalize treatment. He ensured that my appointment went ahead as planned and followed up rigorously post op too. Scar was a bit larger
Mehul Kain
Read More The doctor was helpful. He worked with me to select the best option for treatment and helped finalize treatment. He ensured that my appointment went ahead as planned and followed up rigorously post op too. Scar was a bit larger

